|
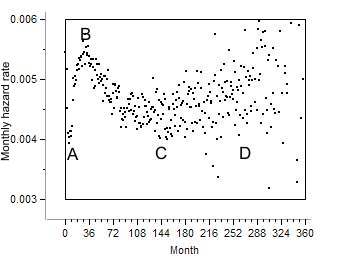
Cancer hazard rates reveal more about cancer biology than any other statistical
function. Hazard rate in breast cancer proceed through three phases. Following
diagnosis and treatment hazard rate rises (AB). By the third year it reaches
its maximum whereupon it declines to a minimum (BC). from there and on it
gradually rises to a second maximum whereupon the patient dies (CD). This
pattern is known as bi-modal hazard (BMH). It is unique to cancer
and does not appear in other chronic diseases. It is an epidemiological hallmark
of cancer. It is so typical of cancer that it distinguishes cancer from other
chronic diseases.
 |
Data source: Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov)
SEER*Stat Database: Incidence - SEER 9 Regs Public-Use, Nov 2004 Sub (1973-2002),
National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics
Branch, released April 2005, based on the November 2004 submission.
Cancer proceeds through two phases, compensated, when the tumor does
not cause any damage or distress, and de-compensated, when the patient suffers. The
first peak and trough (ABC) occur during compensation. The ascending part
(D) accompanies de compensation which ends in death.
The present studies apply hazard rate fractions: HR = #died / (#live at start
of the interval - #lost to follow up)
It is the probability of a patient with breast cancer to die, and is affected
also by other ailments the patient may have.
BMH is the common denominator of the following epidemiological phenomena
1. Recurrence following treatment represented here by the publication
of (Karrison et al (1)
Some other publications describing the same pattern:
The relapse rate
following breast cancer surgery is bi-modal.
(Retsky et al.(2)).
Annual hazard rates of recurrence for
breast cancer after primary therapy are bi-modal (Saphner et al (3))
Mammography paradox: The hazard
following mammography of young females is higher than in controls Cox
(4).
Hazard rates
of recurrence following diagnosis of primary breast cancer
Jatoi et al. (5)
Hazard rate of recurrence of breast
cancer in 3811 spanish patients.
2. Survival following treatment (Ruth
Heimann, Samuel Hellman (6)
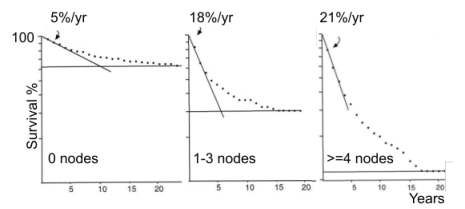
The steep descent is associated with phase AB of BMH, the tapering off with
the BC segment
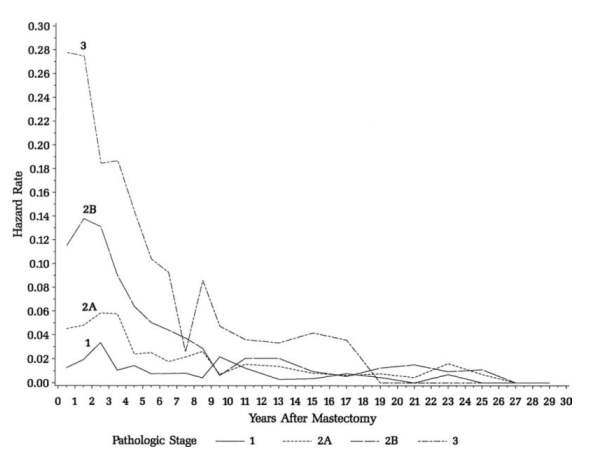
3. Breast cancer recurrence rate Freedman
et al (7)
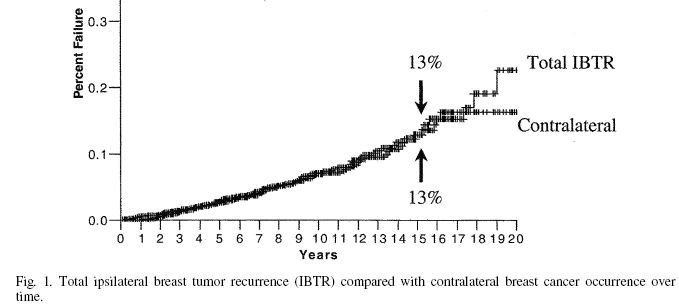
The ascending curve is associated with the BC segment of BMH
4. Cumulative incidence Nielsen et al (8)
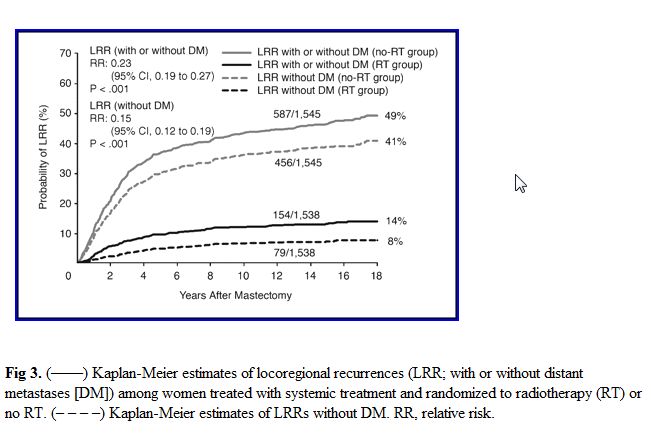
The ascending part is associated with segment AB of BMH. The leveling off,
with the BC segment
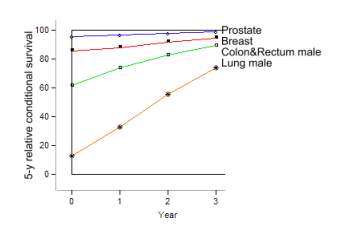
5. Conditional survival
Gloeckler Ries
et al (9)
6. Tumor growth rate is proportional to recurrence
rate
The improving conditional survival is associated with segment BC of BMH.
All these manifestations may be derived from the BMH using
the following relationships:
F(t) - lifetime distribution function
f(t) - the derivative of F(t)
S(t) = 1-F(t) survival function
h(t) = f(t) / S(t) hazard rate
We ought to distinguish between primary hazard or
hazard[death] which accounts for death, depicted in the first curve
and secondary hazards: hazard[recurrence], and hazard[incidence],
which depend on tumor detection and not on death. Survival and conditional
survival may be derived directly from hazard[death]. In order to derive secondary
hazard from primary we need additional information: tumor
growth rate and the resolution power of tumor detecting tools.
Nevertheless all hazard functions point to the same conclusions:
1. AB segment: Hazard rises due to treatment.
2. BC segment: The declining hazard indicates that with time
the patient resists cancer better and better. The longer she lives the better
her chances to survive. The nature of this resistance is the major concern
of this web-site. Although treatment also contributes to this decline, this
phenomenon appears in untreated breast cancer
and in patients who were treated only once and
not treated again later on
The descending portion of BMH appears in all cancers and does not appear in
other chronic diseases.
3. CD segment: Marks the final decline when resources are
depleted and illness overpowers the patient.
Hypothesis
These observations convinced me to propose the following hypothesis.
Cancer is a metabolic deficiency caused by a deficiency of
a yet unknown metabolite A. In order to replenish the missing metabolite the
organism grows a tumor which produces a substitute B. Since
the deficiency continually aggravates, the tumor has to grow more and more
in order to replenish the missing metabolite. In advanced deficiency tumor
destroys vital functions and finally kills the patient. Tumor ablation
aggravates the deficiency and the hazard rises. Patients with micro metastases
are protected from therapy induced total ablation and their hazard rate declines.
Clinically this deficiency is manifested by a wasting disease which starts with weight loss and gradually turns into overt cachexia It is named here pernicious cachexia. The tumor protects against cachexia.
Treatment objectives: Do not treat unless the tumor causes pain and distress or destroys vital functions. Wait as long as cancer is compensated and treat only during de compensation.
Farewell my breast
References
1. Karrison TG,. Ferguson DJ, Meier P. Dormancy of mammary carcinoma after
mastectomy
J. National Cancer Institute, (1999) 91 : 80-85.
2. M. Retsky, R.
Demicheli and W. J.M. Hrushesky
Does surgery induce angiogenesis in breast cancer?
Indirect evidence from relapse pattern and mammography paradox International Journal
of Surgery Volume 3, Issue 3
, 2005, Pages 179-187
3.
Saphner T, Tormey DC, Gray
R.
Annual hazard rates of recurrence for breast
cancer after primary therapy J
Clin Oncol 1996; 14: 2738-2746.
4. Cox B, Variation
in the effectiveness of breast screening by year of follow-up, J Natl Cancer
Inst Monogr 22 (1997), pp. 6972
5. Ismail Jatoi , Anna Tsimelzon , Heidi Weiss , Gary M. Clark and Susan G.
Hilsenbeck
Hazard rates of recurrence following diagnosis of primary breast cancer
Breast Cancer Research and Treatment 2005; 89: 2; 173-178
6. Ruth Heimann, Samuel Hellman
Clinical Progression of Breast Cancer Malignant Behavior: What to Expect and
When to Expect it.
Journal of Clinical Oncology, Vol 18, Issue 3 (February), 2000: 591
7. GARY M. FREEDMAN, M.D., PENNY R. ANDERSON, M.D., ALEXANDRA L. HANLON, M.S.,
PH.D.,DEBRA F. EISENBERG, M.S., AND NICOS NICOLAOU, M.D.
PATTERN OF LOCAL RECURRENCE AFTER CONSERVATIVE SURGERYAND WHOLE-BREAST IRRADIATION
Int. J. Radiation Oncology Biol. Phys., Vol. 61, No. 5, pp. 1328–1336,
8. Hanne M. Nielsen, Marie Overgaard, Cai
Grau, Anni R. Jensen, Jens Overgaard
Study of Failure Pattern
Among High-Risk Breast Cancer Patients With or Without Postmastectomy
Radiotherapy in Addition to Adjuvant Systemic Therapy: Long-Term Results From
the Danish Breast Cancer Cooperative Group DBCG 82 b and c Randomized Studies
Journal of Clinical
Oncology, Vol 24, No
15 (May 20), 2006: pp. 2268-2275
9 Lynn A. Gloeckler Ries,
Marsha E. Reichman, Denise Riedel Lewis, Benjamin F. Hankey, Brenda K. Edwards
Cancer
Survival and Incidence from the Surveillance, Epidemiology, and End Results
(SEER) Program
The Oncologist, Vol. 8, No. 6, 541–552, December 2003